If my urine reacts positive for sugar I've got diabetes. If my pregnancy test is positive I'm pregnant. How can anyone be HIV positive and not have HIV?
A1. "HIV positive" is an abbreviation for "HIV antibody positive". The test which is universally used [1] to diagnose HIV infection is not culture and detection or isolation of an actual virus or a virus particle from the blood or tissues. Rather it is a test performed on a specimen of the patient's blood [2] where the test kit registers the presence of antibodies. So the question needs to be rephrased. "Are the antibodies detected in your test caused by infection with HIV?" That is what is meant by the term "HIV antibodies".
Q2. What are antibodies?
A2. Antibodies are proteins made by cells called lymphocytes. Each lymphocyte is responsible for the manufacture of one and one only unique antibody molecule. When it is stimulated it and its clones make millions of the same molecule over and over again. The body has a repertoire of approximately one million antibodies and antibody production is switched on when something foreign such as a bacterium or virus or protein is introduced into the body. The agents and substances that turn on the production of antibodies are collectively referred to as antigens (from ANTIbody GENerating). The most powerful antigens are proteins especially when introduced directly into the blood stream. The antigen in effect "chooses" one of the million antibodies by virtue of a complementary chemical makeup between the antigen and antibody. In immunological language [3] the antibody "recognises" and is "directed against" its particular antigen. An analogy is parents waiting to pick up their children after school. Parents and children go off together because particular sets of children and parents are "directed" to each other because of mutual recognition.
The chemical make which underpins antigen/antibody "recognition" also means that an antibody and its antigen react together. Thus when say measles virus protein and antibody are mixed in a test tube they unite via a chemical bond to form an antibody/protein complex. This results in a precipitate which turns the solution a different colour. The intensity of the colour change can be measured to make the reaction quantitative. This is how an ELISA works except the proteins are "HIV" and not measles.
Q3. So HIV antibodies react with HIV proteins?
A3. Yes assuming HIV exists.
Q4. If an antibody is discovered in my blood that reacts with the HIV proteins, does this prove it is an HIV antibody?
A4. No. That is what this discussion is all about.
Q5. Could it be an HIV antibody?
A5. Yes again provided there is proof for the existence of HIV. But it could also be a "non-HIV" antibody.
Q6. How can an antibody react with an "HIV" protein and not be an HIV antibody? It seems like a contradiction in terms.
A6. There is a lot more to proving antibodies are "HIV antibodies" than putting words next to each other in a sentence. Antibodies directed against one protein (with which they react) may also react with another, different protein against which that antibody is not directed. The latter is known as a "cross-reaction". The problem is that all we see in the test tube is a reaction. Either the solution changes colour or it doesn't. When there is a reaction we can't tell whether it is due to a genuine antibody antibody or a cross reacting "non-genuine" antibody. This kind of thing is not a big deal. For example, chlorine reacts with sodium to form a white powder. But bromine also reacts with sodium to form bromine to form a white powder. And both taste salty. We aren't in the least surprised that two different substances react with the same something else. And no one would pretend for a moment a substance can be identified as chlorine because it reacts with sodium to form a white powder.
Q7. What is the basis of cross-reactions?
A7. It has a chemical basis. When antibodies react with proteins they only react with a relatively small portion of the total protein molecule. As we've said elsewhere, it's like hugging your grandmother. Or kissing your wife or husband. You and your grandmother or partner are not in contact over 100% of your body surfaces. The part of the antigen that does the reacting is known as the "antigenic determinant" or "epitope" [4]. This small portion is only a few percent of the total but sometimes another otherwise different protein shares the same or nearly the same portion. Since this is the "business end" of the antigen the same antibody reacts with it. The antibody can't tell the difference.
Q8. Are cross-reactions part of real life laboratory tests or are they just something theoretical the Perth Group like to talk about to make people doubt the validity of the HIV tests?
A8. Cross-reactions are not theoretical. They plague all attempts at serological diagnoses. That is why antibody tests are likened to attempts to determine the shapes of clouds by analysing the shadows they cast on the ground. To see how cross-reactions feature go to PubMed and do a search using the words "milk AND proteins AND cross-reaction". One of the papers that comes up is:
"Cross-reactivity between mammalian proteins. Restani P, Beretta B, Fiocchi A, Ballabio C, Galli CL.
Laboratory of Toxicology, Department of Pharmacological Sciences, University of Milan, Milan, Italy. patrizia.restani@unimi.it"
The abstract of this paper says "...antibodies specific for cows milk proteins are able to recognize the major part of milk proteins from mammals bred in Mediterranean countries (sheep, goat, and buffalo); weak cross-reactivity was observed with milk proteins from mares and donkeys. None of the antibodies used in our studies reacted with proteins from an exotic mammalian species: the camel".
This tells us that antibodies directed against cows milk proteins also react with sheep, goat and buffalo milk proteins. Although these are different proteins from other species of animals. Now imagine you want to test a person for antibodies to sheep milk. You could be a doctor with a patient who believes drinking sheep milk is more healthy than cows milk but in whom you suspect an allergy to sheep milk has developed. You want to know if that person is producing antibodies to sheep milk that cause this allergy. To find out you take some sheep milk, obtain the proteins and to these add some serum from the patient. You see a reaction between the patient's antibodies and the sheep milk proteins but what can you conclude? Is this reaction proof the patient has antibodies to sheep milk? Could this person be "infected" with sheep milk? The reaction could certainly indicate exposure to sheep milk. But because you know that cows milk antibodies also react with sheep milk proteins it could equally be due to cows milk antibodies. How can you say which antibody it really is? There will be a reaction no matter which antibody is added to the sheep milk because (a) the sheep antibody will react with sheep milk and (b) the cows antibody will react with sheep milk. So it is impossible to identify the "genuine" sheep antibody on the basis of a reaction with sheep milk [5]. If the sheep milk protein was an HIV protein and you added some serum and saw a reaction you would not be able to distinguish between a genuine "HIV" antibody and a genuine "non-HIV" antibody. This is why finding antibodies which react with "HIV" is not proof they are "HIV" antibodies. Serology is not that simple but how many HIV positive people have been told about the phenomenon of antibody cross-reactivity?
Q9. Milk is one thing and HIV is another. Does the Perth Group have any data on antibodies that react with HIV which aren't HIV antibodies?
A9. There are considerable data on this topic. In Australia for example 25% of healthy individuals have at least one antibody that reacts in the HIV Western blot test. Since on average 0.1% of Australians are said to be "infected" with HIV virtually all these antibodies must be "non-HIV" cross-reacting. In fact experts such as Anthony Fauci teach medical students that "HIV" Western blots which are not positive because they lack "sufficient" antibodies ("bands" see here) to be classified positive are caused by cross-reacting antibodies. Before we mentioned measles which also provides a good example of cross-reactivity. In a study of acute measles infection in non-HIV infected children and young adults reported from the USA and Peru, 43/75 (62%) developed antibodies which reacted with one or more of the "HIV" proteins. In 1995 in Africa there were 551,000 childhood deaths from measles and awareness of this problem may explain why, in one African study of HIV infection, “Children hospitalized with measles were excluded”.
Q10. Does this mean you can never use antibody tests to diagnose infections?
A10. No. What it means is you must have a way of sorting out which reactions are caused by "real" antibodies and which are due to cross-reacting "pretenders". The only way to do that is by validating the reactions against what you are looking for. In other words, it comes down to an empirical process. We talk about this at length in many of our papers. You determine the number of positive tests in people you know are infected. But you have to prove infection by some other means apart from the antibody test. Which can only be HIV itself. By isolating it. You can't use the antibody test for verification because you would be validating the test against itself. That is not permitted. Then you determine the number of negative tests in people not infected. That is in people who, despite your best efforts, you cannot isolate HIV. If the tests are highly specific for HIV (as the HIV experts claim they are) then positive tests must be virtually the exclusive domain of people from whom HIV could be isolated. People from whom HIV could not be isolated should almost never test positive. If your data proves these two things then you have a very good test which you can now put to general use.
Q11. If you have to go to all this trouble why not test for HIV directly in the first place? Why bother with antibodies?
A11. Because antibody tests are far simpler and much cheaper than isolating viruses. And their use is quite legitimate providing they are proven specific against the virus in a large number of people before introducing the test into routine clinical practice. Unfortunately an evaluation against HIV itself has never been reported in the scientific literature. That is why we argue no one knows how many "HIV" positive people are infected with HIV. It could be all or it could be none. The failure to address or even acknowledge this most basic scientific problem may have tragic consequences.
Q12. But why would AIDS patients or people who are at risk of AIDS have cross-reacting antibodies rather than true HIV antibodies?
A12. Because what characterises the AIDS risk groups is exposures to many and varied foreign substances all capable of stimulating the production of antibodies. Such as blood or blood products or germs or semen or drugs. In fact AIDS patients have elevated levels of antibodies directed against all manner of antigens which are not "HIV". And the more antibodies one has the more likely one or several will cross-react with "HIV". This is borne out by the fact that high levels of antibodies predict a positive test for "HIV".
Q13. So if I'm HIV positive it may not mean I have a retrovirus infection and I don't have to worry about getting sick?
A13. No. There is no doubt that in the AIDS risk groups these antibodies, wherever they come from, whatever produces them, indicate something may be wrong or about to go wrong with your health. We can say this because there are many studies showing that "HIV" positive individuals are statistically at increased risk from having or developing certain diseases [6]. That's not to say all HIV positive people will get sick or develop AIDS. What the Perth Group have been arguing for many years is that to date there is no proof the test is positive because of antibodies directed against a retrovirus HIV. Even if there is a retrovirus HIV. Obviously there has to be an explanation for the existence of these antibodies but we don't need to know what that is in order to prove they signal an increased likelihood of ill health. Just as we don't have to know the cause of a fever to know fever predicts the likelihood of ill health. Both these correlations are well established and are sufficient proof.
Q14. What about healthy people who are not in an AIDS risk group? What does a positive test mean for them?
A14. Unfortunately, when it comes to healthy people who are not in an AIDS risk group, the predictive power of a positive test is less certain. The only way to determine that risk is to compare the health of a large group of "HIV" positive and "HIV" negative healthy individuals over several years. However, all this would have to be done in secret. If the individuals or their relatives or their doctors know the test results this would bias the experiment. For example, the "HIV" positives might believe they are going to die and their doctors would feel obliged to offer them "anti-HIV" drugs which themselves are toxic and might result in illness. It is far too late for this experiment to take place. There is further discussion on non-specificity and the meaning of "HIV" positive in our Mother to Child Monograph here (search for "ESR" on page 14) and read what we said here.
Q13. So what should an HIV positive person do if he or she is reluctant to accept it means HIV infection?
A13. The Perth Group does not advise patients on medical treatments. That is solely a matter for patients and their doctors. However, since it is known that exposure to rectal semen (in both men and women) and drugs as well as fungal and mycobacterial diseases can result in antibodies which react in the "HIV" antibody tests, it makes good sense to avoid these exposures and to have all diseases properly evaluated and treated.
ENDNOTES
"Universal" is not quite right. One of the several "Great AIDS Mysteries" is the CDC recommendations for diagnosing HIV infection:
"In adults, adolescents, and children infected by other than perinatal exposure, plasma viral RNA nucleic acid tests should NOT be used in lieu of licensed HIV screening tests (e.g., repeatedly reactive enzyme immunoassay)” (emphasis in original).
But, “HIV nucleic acid (DNA or RNA) detection tests are the virologic methods of choice to exclude infection in children aged <18 months” (“Positive results on two separate specimens)
Reference: Centers for Disease Control and Prevention. Mortality and Morbidity Weekly Reports 1999;48 (RR-13):1-27, 29-31. See here
This means that antibody tests are to be used to diagnose HIV in everyone except babies < 18 months old. But, in such babies RNA or DNA is to be used although the same test cannot be used to diagnose HIV in everyone else. Yet such RNA or DNA is, according the HIV experts, unique and specific to a retrovirus HIV. We may wonder what is going on? Try emailing the CDC and seeking clarification.The test is performed on serum. That is the amber coloured fluid that separates from blood after it clots. Antibodies (and much more) are dissolved in the serum. Hence a positive test is sometimes called "seropositive".
Language has a power all its own. Immunologists make liberal use of metaphor especially military metaphor. Immunologists talk of the "soldiers" of the immune system, "killer" lymphocytes and antibodies "going into battle" to "defeat the invader". "Anti"-body has the same connotation. The word "recognise" is also an attempt to anthropomorphise certain facets of the immune system. The only means to "recognise" anything is by memory. That is how parents and children know who goes home with who. If antibodies and antigens "recognise" one another then we might as well say that sodium and chlorine react to form sodium chloride (table salt) because they also "recognise" one another. Chemists do not use this language because it an attributes a property to chemical substances which has no basis in reality. Antibodies and antigens, like sodium and chorine, react because they can. Even if they have never "met" before. There are more exotic thermodynamic explanations but essentially that is all there is to it.
Epitope: Etymology: International Scientific Vocabulary, from epi- + Greek topos place Date: 1960--a molecular region on the surface of an antigen capable of eliciting an immune response and of combining with the specific antibody produced by such a response -- called also determinant, antigenic determinant
You can demonstrate "cross-reactivity" with some kitchen chemistry. You are unlikely to have a supply of cows or sheep milk antibodies but in their place you can substitute vinegar and lemon juice. These are different chemically (as are antibodies) but are both acidic and curdle milk proteins (as do antibodies). We will imagine that the vinegar is cow antibody and the lemon juice is sheep antibody. To carry out the experiment you will need to obtain a small amount of sheep milk. (Or you can imagine cows milk is sheep milk). Put a tablespoon of sheep milk in a saucer and add a teaspoon of 'sheep antibody' (lemon juice). Into a second saucer of sheep milk add a teaspoon of 'cow antibody' (vinegar). Gently rock the saucers to mix the reactants and then drain off the remaining liquid to confirm agglutination of the milk proteins. BOTH saucers contain agglutinated milk (both sheep and cows milk antibodies react with sheep milk). Demonstrate this experiment to another person and ask him to nominate to which saucer was vinegar was added and to which lemon juice added. He cannot. It is impossible.
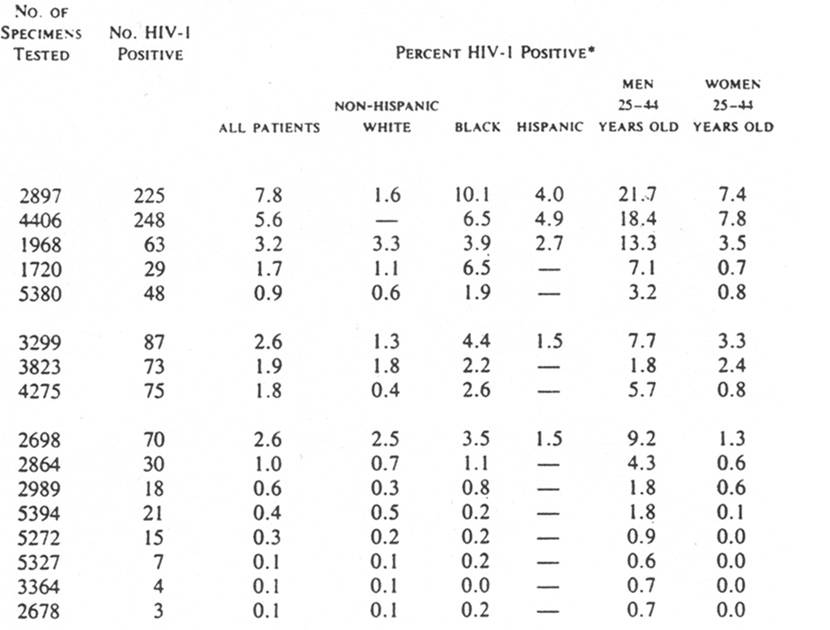
This does not just apply to sickness due to the "AIDS" diseases. In 1990 St. Louis and his colleagues reported that amongst 89,547 anonymously tested blood specimens from 26 US hospital patients at no risk of AIDS, between 0.7% to 21.7% of men and 0-7.8% of women aged 25-44 years were found to be HIV WB positive. It is important to note that this study not only excluded patients from the known AIDS risk groups but also those with even meagre HIV/AIDS risks including "gunshot and knife wounds, conditions which have been reported to be associated with a higher than expected rate of HIV-1 seroprevalence" [7]. They also found that at the five hospitals with the highest rates of "HIV" antibodies, one third of positive tests were in women. Yet men vastly outnumber women as AIDS patients. Thus unless hospital patients judged at no or meagre risk of AIDS are wrongly classified, "sickness" (the reason people attend hospitals) itself must be the cause for cross-reacting antibodies which react in the "HIV" tests. This is not an unexpected finding and is further reason to argue "HIV" antibody tests are non-specific. It is not beyond the realm of possibility that the only difference between the individuals reported in the St. Louis study and individuals tested in Africa is that more of the latter are sicker (with even more likelihood of cross-reacting antibodies) but are very unlikely to be found inside a hospital. The African serological data may represent nothing more than a gigantic St. Louis study group. See here to see some of the St. Louis data. In other words, to explain the high prevalence of positive antibody tests in Africa one only need to know that Africans are subject to many diseases such as fungi and mycobacteria which of their own accord result in antibodies which are known to cross-react in the "HIV" antibody tests. There is no need to postulate the activity of an immunodeficiency retrovirus because Africans are already immune deficient by virtue of their illnesses. Such as tuberculosis and many parasitic diseases. What is spreading in Africa is not a retrovirus but "HIV" testing.
St Louis ME, Rauch KJ, Petersen LR, Anderson JE, Schable CA, Dondero TJ. Seroprevalence rates of human immunodeficiency virus infection at sentinel hospitals in the United States. The Sentinel Hospital Surveillance Group. New England Journal of Medicine 1990;323(4):213-8.
{kind=link}